We do not diagnose disease or recommend a treatment protocol or dietary supplement for the treatment of disease. You should share this information with your physician who can determine what nutrition and disease treatment regimen is best for you. Ask your physician any questions you have concerning your medical condition.
You can search this site or the web for topics of interest that I may have written (use Dr Simone and topic). “We provide truthful information without emotion or influence from the medical establishment, pharmaceutical industry, national organizations, special interest groups or government agencies.” Charles B Simone, M.MS., M.D.
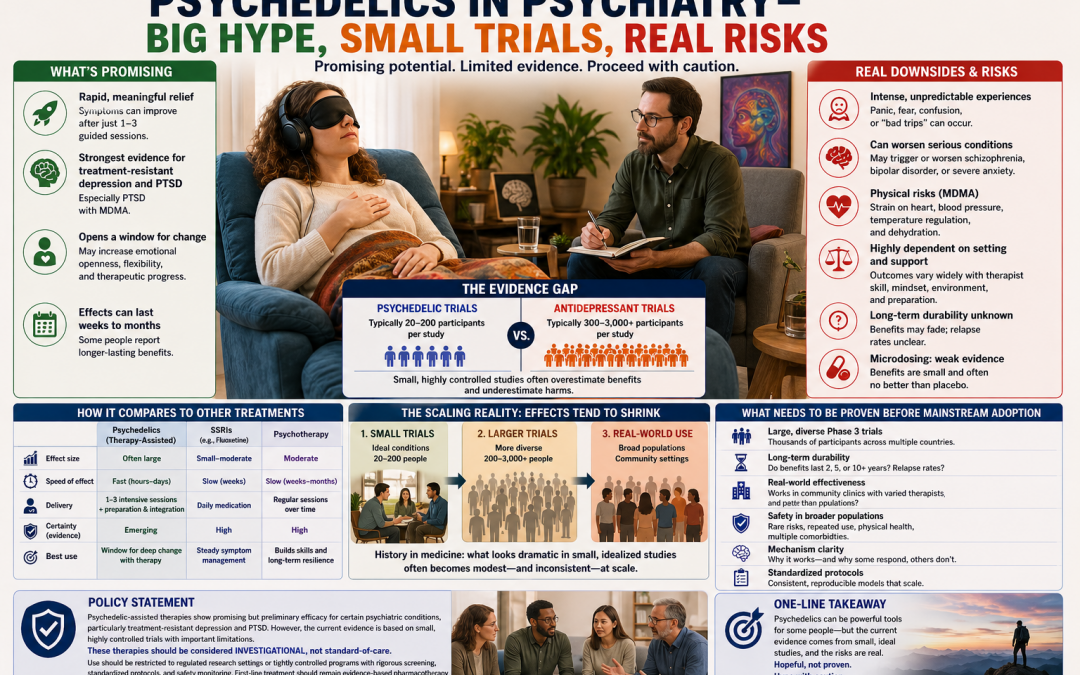
PSYCHEDELICS IN PSYCHIATRY — BIG HYPE, SMALL TRIALS, REAL RISKS
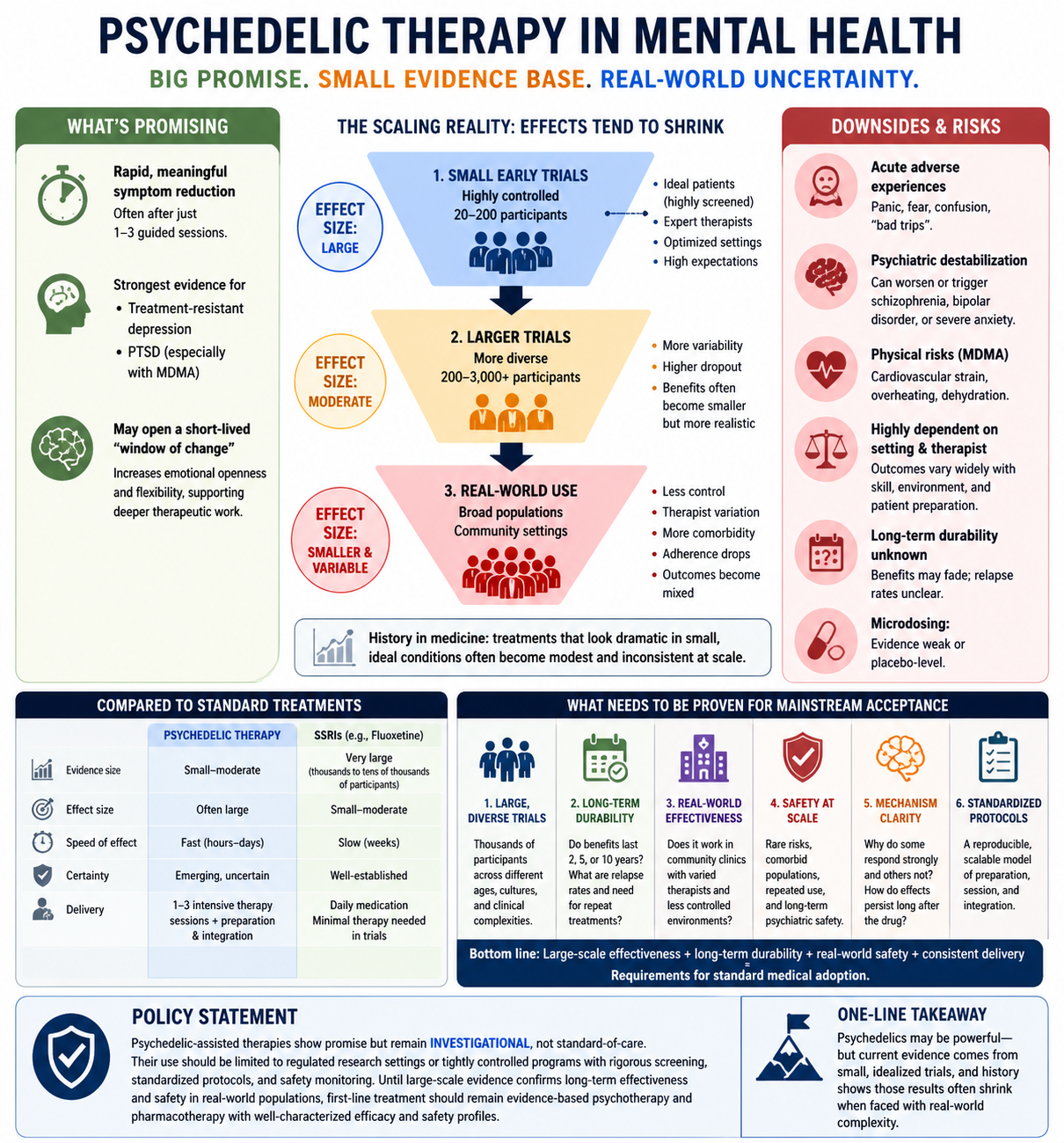
Bottom line: Psychedelic-assisted therapy (e.g., psilocybin, MDMA) shows striking early results—but those results come largely from small, highly controlled studies that tend to overstate benefits and underrepresent real-world risks.
What’s promising
Rapid, sometimes large symptom reductions in treatment-resistant depression and PTSD
Effects can appear after just 1–3 guided sessions
May open a short-lived “window” for deeper therapeutic work
Where the evidence is weak
Small trials dominate (often 20–200 participants) vs. thousands for drugs like fluoxetine
Highly selected patients (healthier, motivated, screened out for risk)
Intensive support that’s difficult to replicate at scale
Blinding problems—participants usually know they received the drug, inflating expectations and outcomes
Implication: Early effect sizes are likely overestimated and may shrink substantially in larger, real-world studies.
Downside risks (often underemphasized)
Psychiatric destabilization: can worsen or trigger schizophrenia, bipolar disorder, or severe anxiety
Typical pattern in medicine: Small trials → large effects → bigger trials → smaller, more variable effects → real world → further dilution
Compared to standard treatments
SSRIs (e.g., fluoxetine): modest effects, but robust, large-scale evidence and predictable safety
Psychedelics: larger early effects, but lower certainty, harder to standardize, and more variable outcomes
Policy stance
Psychedelic therapies should be considered investigational, not standard care. Broader adoption requires:
Large, diverse Phase 3 trials
Multi-year durability data
Clear safety profiles in real-world populations
Standardized, scalable treatment protocols
One-line takeaway
Psychedelics may be powerful—but current evidence is built on small, idealized trials, and history suggests those results often don’t hold when exposed to the complexity of real-world medicine.
Policy Statement: Psychedelic-Assisted Therapies in Mental Health
Psychedelic-assisted therapies, including psilocybin- and MDMA-based interventions, demonstrate promising but preliminary efficacy for certain psychiatric conditions, particularly treatment-resistant depression and post-traumatic stress disorder. However, the current evidence base is derived predominantly from small, highly controlled clinical trials with carefully selected participants, intensive therapeutic support, and methodological limitations (including challenges with blinding and expectancy effects).
Given the well-established tendency of small trials to overestimate treatment effects and the uncertainty surrounding long-term durability, safety in broader populations, and real-world scalability, these therapies should be classified as investigational rather than standard-of-care.
Clinical use, if pursued, should be restricted to regulated research settings or tightly controlled programs with rigorous patient screening, standardized protocols, and comprehensive safety monitoring. Widespread adoption should be deferred pending:
Demonstrated effectiveness in real-world clinical environments
Clear safety profiles across diverse and comorbid populations
Until such evidence is established, first-line treatment should remain evidence-based pharmacotherapy and psychotherapy with well-characterized efficacy and safety profiles.
The federal government spends 27% of your taxes on healthcare, which is the most expensive part of the federal budget. Let’s not add to it.