

We do not diagnose disease or recommend a treatment protocol or dietary supplement for the treatment of disease. You should share this information with your physician who can determine what nutrition and disease treatment regimen is best for you. Ask your physician any questions you have concerning your medical condition.
You can search this site or the web for topics of interest that I may have written (use Dr Simone and topic).
“We provide truthful information without emotion or influence from the medical establishment, pharmaceutical industry, national organizations, special interest groups or government agencies.” Charles B Simone, M.MS., M.D.
CHILDREN SHOULD NOT GET THE “VACCINE”
“ABOVE ALL DO NO HARM”
Written November 21, 2021 https://bit.ly/3nB4CyK
SUMMARY
Children have very few ACE2 receptors on their cells. The SAR-CoV2 (COVID-19) virus requires ACE2 receptors to attach and infect cells. This is why children rarely get infected, have a low risk of becoming ill, a low risk of spreading the virus to other children or adults, and an almost zero risk of dying from it.
However, the “vaccine” shots contain highly inflammatory Lipid Nanoparticles (LNP) that encapsulate the mRNA. It is known that the Lipid mRNA Nanoparticle complexes have intrinsic toxicity above and beyond that associated with the spike in all ages but especially children leading to multiple organ damage of the brain, heart, coagulopathy, reproductive systems (preferentially to ovaries) and immune systems.
The shot cripples children’s natural protective innate immunity. The children’s cells are then forced to make spike proteins that can cause inflammation and organ dysfunction when they bind to the few ACE2 docking sites on their cells of the Mucus Membranes, Eye, Respiratory Tract, Heart / Blood Vessels, Brain, Musculoskeletal, Reproductive organs, Gastrointestinal, Kidney, Skin. The spike also binds to and renders the p53 gene ineffective. The p53 gene is a tumor suppressor gene that stops the formation of tumors.
And the efficacy of the mRNA “vaccine” is more in doubt, as shown in a recent letter to the Lancet Regional Health by Gunter Kampf who provided data showing that the vaccinated are now as likely as the unvaccinated to spread disease. He concluded: “It appears to be grossly negligent to ignore the vaccinated population as a possible and relevant source of transmission when deciding about public health control measures.”
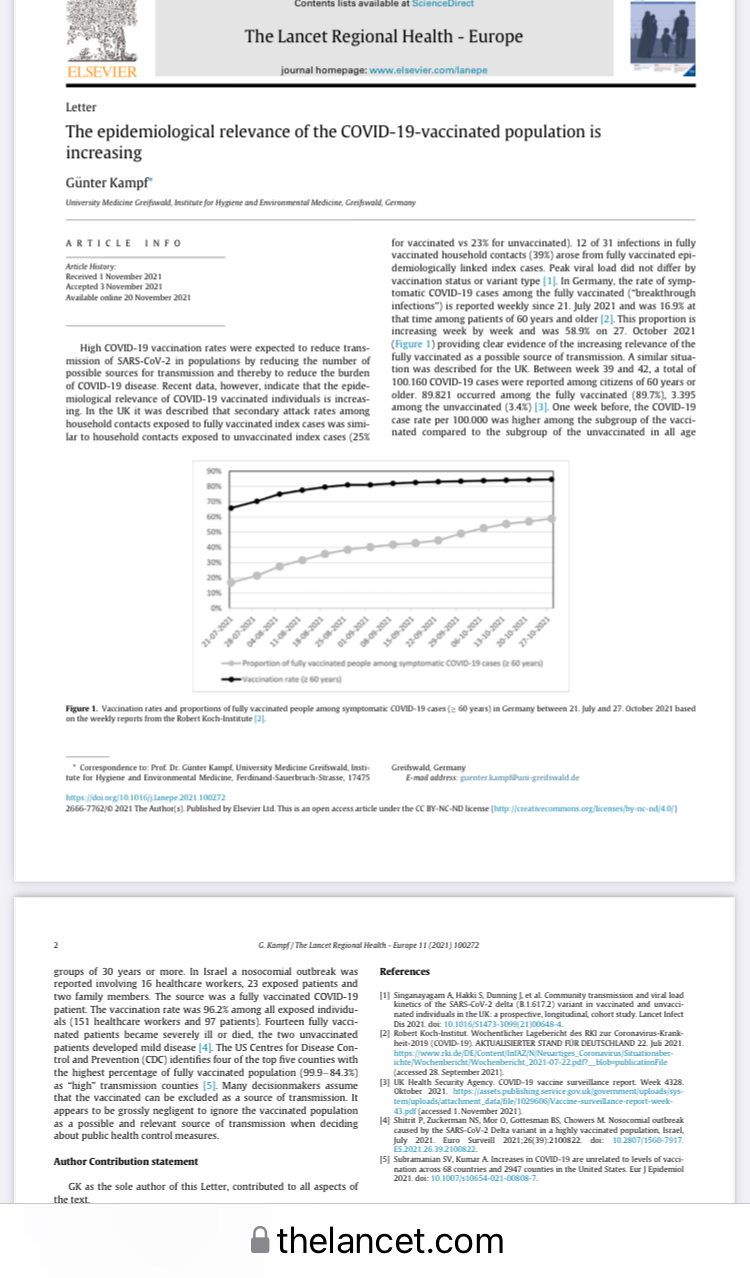
https://www.thelancet.com/action/showPdf?pii=S2666-7762%2821%2900258-1
Physicians take the Hippocratic Oath and pledge “Above All Do No Harm.” The “vaccine” poses great risk of harm to children.
CHILDREN HAVE VERY FEW ACE2 RECEPTORS
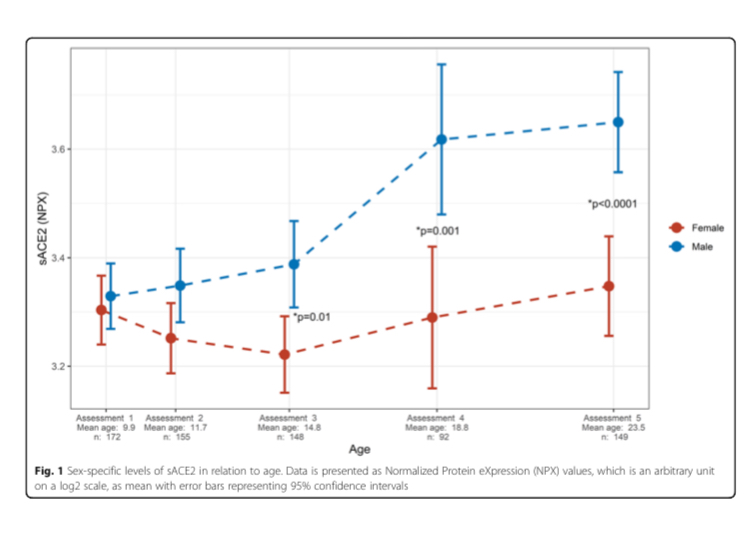
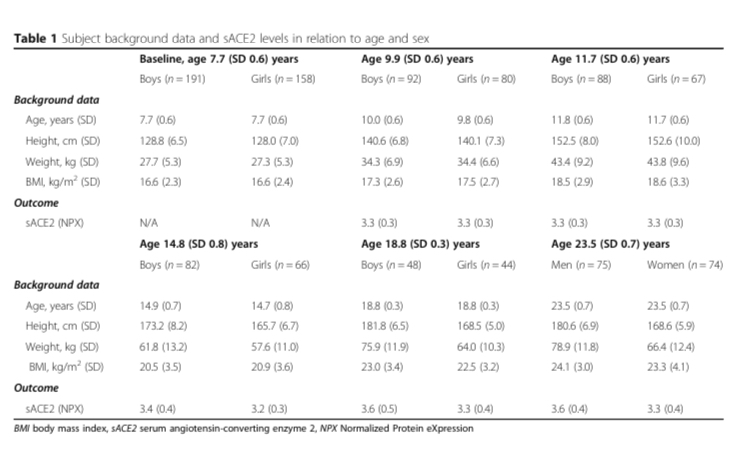
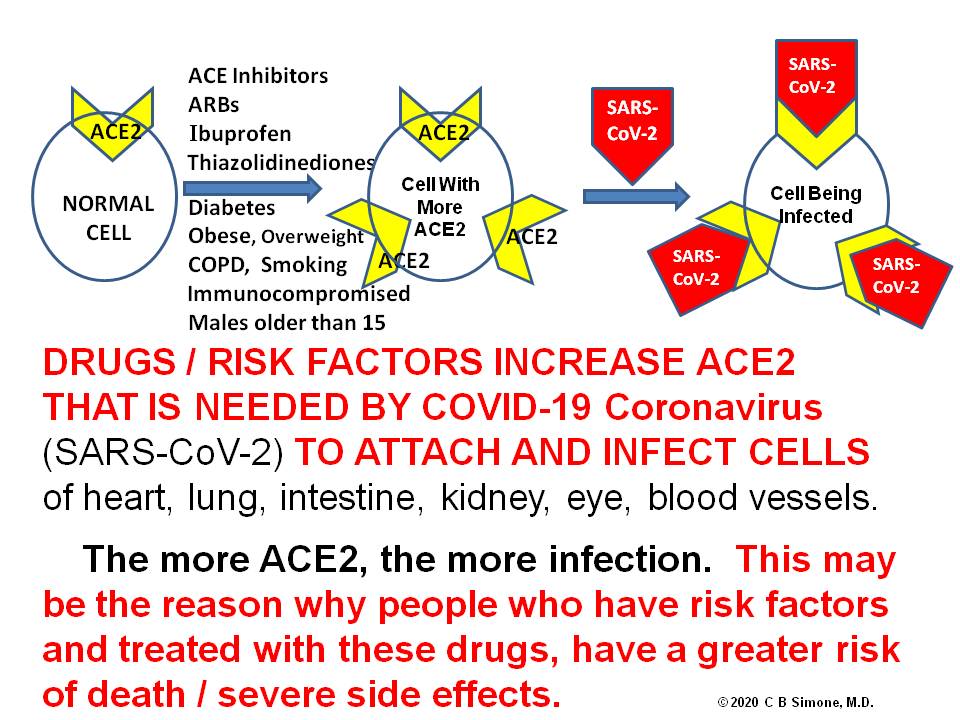
Young children have very few ACE2 receptors in the nasal passage cells and upper respiratory airways and therefore have little risk of getting infected or becoming very ill, and less likely to spread the virus to others because COVID 19 needs ACE 2 receptors to attach and infect cells. Girls entering puberty have rising estrogens that suppress the renin-angiotensin system and therefore results in fewer ACE2 receptors, but boys entering puberty have rising testosterones that increase ACE2 receptors.
During infection an enzyme (ADAM-17) can cleave off the cell’s membrane ACE2 resulting in shedding of ACE2 in the blood (soluble ACE2). Soluble ACE2 can reflect the amount of cell membrane ACE2. The more ACE2, the more infection, the more organ dysfunction.
https://ccforum.biomedcentral.com/track/pdf/10.1186/s13054-020-02942-2
Renin angiotensin system and gender differences in the cardiovascular system https://academic.oup.com/cardiovascres/article/53/3/672/327796
In another study of 305 patients, 185 older children (10-17 years old), 46 young adults (18-24 years old), and 29 adults (≥25 years old) all had higher expression of ACE2 in the nasal epithelium compared with 45 younger children (4-9 years old).
The injected “vaccine” bypasses this natural protection of very few ACE 2 receptors
The more ACE2 receptors there are in a person, the more spike proteins get attached leaving fewer spike proteins freely available to make antibodies. That’s why people who take certain medicines and/or have certain risk factors have a blunted immune response to the vaccine but still can have inflammation and organ dysfunction.
https://jamanetwork.com/journals/jama/fullarticle/2766522 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30937-5/fulltext https://www.francesoir.fr/opinions-tribunes/pourquoi-la-proteine-spike-est-toxique-dans-le-covid-19-et-aussi-dans-les-vaccinshttps://pubmed.ncbi.nlm.nih.gov/33360731/
Factors other than ACE2 that might protect children include: (1) differences in innate and adaptive immunity; (2) more frequent recurrent and concurrent infections; (3) pre-existing immunity to coronaviruses; (4) differences in microbiota; (5) higher levels of melatonin; (6) protective off-target effects of live vaccines, and (7) lower intensity of exposure to SARS-CoV-2.
Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections https://adc.bmj.com/content/106/5/429
99.995% Survive a COVID-19 Infection
COVID-19 poses almost a zero risk to children – 99.995% survive a COVID-19 infection, fewer than two out of every million children died with COVID. These statistics are well known to the CDC, NIH, and FDA.
(Lancet https://www.thelancet.com/journals/lanchi/article/PIIS2352-4642(21)00066-3/fulltext)
 COVID-19 Deaths per capita by age in the United States
COVID-19 Deaths per capita by age in the United StatesFrom more than 700 medical papers and 47 full texts we know:
Children have a very low risk of spreading the infection to other children or adults.
Children have a low risk of bringing the virus home or becoming ill and/or dying
2 million children in school in Sweden with no mask mandates – zero deaths from Covid and a few instances of transmission and minimal hospitalization.
No instances of asymptomatic spread from positive asymptomatic cases among all 1,174 close contacts of the cases, based on a base sample of 10 million persons. (Nature)
https://pubmed.ncbi.nlm.nih.gov/32430964/https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7821981/
https://www.nature.com/articles/s41467-020-19802-whttps://www.aier.org/article/why-we-must-not-be-forced-into-vaccinating-our-children-from-covid-beware/
Fully vaccinated people can harbor, shed, spread the virus to others, and get breakthrough reinfection. Fully vaccinated and unvaccinated people can have high viral loads and both are equally infectious.
CDC Admits It Doesn’t Collect Data on People Naturally Infected with COVID becoming re-infected or transmitting the virus to others.
“VACCINE” DOES NOT PREVENT INFECTION OR TRANSMISSION
The “VACCINE” does not prevent viral infection and it does not prevent viral transmission.
CHILDREN HAVE STRONGER INNATE IMMUNITY
Children, compared to adults, have stronger antiviral innate immunity to SAR-CoV2.
The immune system has two categories: 1) the innate or nonspecific immunity; and 2) the adaptive or specific immunity, which recognizes specific microorganisms or antigens previously seen.
The innate immune system is the first line of defense and is intended to prevent infection and attack the invading pathogens very quickly (minutes to hours).
Innate immunity has multiple components: physical barriers (skin, mucous membranes, mucus); cell enzymes (lysozyme), white blood cells that destroy invaders (neutrophils, monocytes, macrophages), inflammation-related proteins (complement, C-reactive protein), and cells that release cytokines and inflammatory molecules (i.e., macrophages, mast cells, natural-killer cells). When an invader is detected signals are sent to prevent infection, destroy the invader, and stimulate the immune system.
Compared to adults, children’s innate immune systems have high levels of interleukin 17A (IL-17A) and interferon gamma (INF-g) which mobilizes the immune system during early infection and combats viral replication, respectively.
However the mRNA shots:
1) cripple the innate immunity by suppressing InterleukinFN-α (type 1) signaling cascade that can cause the reactivation of latent viral infections and the reduced ability to fight off future infections. This does not happen with natural infection.
2) hide the mRNA from our defenses, promote a longer biological half-life for the spike proteins, and cause higher spike protein production.
3) disturb protein synthesis and cancer surveillance with a link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage.
4) induce immune cells to release large quantities of exosomes containing spike protein along with critical microRNAs that induce signals at distant sites producing serious inflammation.
https://d197for5662m48.cloudfront.net/documents/publicationstatus/75311/preprint_pdf/7204e73a5bc787e851c8d15a3e538ec7.pdf
B CELLS MAKE ANTIBODIES
B cells make antibodies – and children, because they are exposed to several coronaviruses in early childhood, are better protected against this coronavirus – SARS-CoV 2.
T CELLS
T Cells – young children have mostly untrained T cells that can respond rapidly to novel viruses.
WHAT HARM DO THE SHOTS POSE?
First, the U.S. Patent Office recognizes the word “vaccine” to be a “compound which prevents infection.” These shots do not prevent infection.
But on November 4, 2021 the CDC changed its definition of “VACCINE” to justify its needs. Vaccine was originally defined as “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.” NOW, “A preparation that is used to stimulate the body’s immune response against diseases.”
The Vaccine Adverse Events Reporting System (VAERS) is a surveillance system managed by both the CDC and FDA. VAERS has been shown to report about 1% of actual vaccine/inoculation adverse events.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7581376/
In a June 2021 analysis of VAERS COVID-19 vaccine death reports Scott Mclachlan of the University of London found that “contrary to claims that most of these reports are made by lay-people and are hence clinically unreliable,” health service employees were the reporters at least 67 percent of the time, and “there were only 14 percent of the cases for which a vaccine reaction could be ruled out as a contributing factor in their death.”
And generally, the FDA issues a Black Box warning if there are 10 deaths attributed to a vaccine or drug, and if there are more than 50 deaths, the drug is taken off the market.
The data satisfy all five of the Bradford Hill criteria, a framework scientists use to determine whether one thing is causing another. In this case, because COVID-19 vaccination data satisfies the Bradford Hill principles, the reported deaths are highly likely caused by COVID-19 vaccinations.
January 24, 2022 – at Senator Ron Johnson’s hearing COVID-19 A Second Opinion, Attorney Thomas Renz testified that data from the Military’s Defense Medical Epidemiology Database DMED revealed that the vaccines cause an increase of: 300% Miscarriages, 300% Cancer, 487% Breast Cancer, 369% Testicular Cancer, 2100% Hypertension, 1048% Neurological Disorders (82k to 863k), 290% Bell’s Palsy, 155% Birth Defects, 468% Pulmonary Embolism, 269% Myocardial Infarction, 300% Tachycardia, 450% Migraines, 470% Female Infertility, 437% Ovarian Dysfunction.
Renz testified that “DOD & CDC withheld vaccine surveillance data since Sept 2021.”
After Renz, attorney Leigh Dundas testified that Department of Defense changed data in DMED to conceal cases of myocarditis in vaccinated service members. The military whistleblowers reported a DMED search of “acute myocarditis”: 1,239 cases in Aug 2021, but the same search in Jan 2022 had only 307.
May 13, 2022:
COVID Vaccine Adverse Events Reported (CDC) 1,268,008
Deaths 28,141
Of those deaths, 7,382 (28.8%) occurred on day 0, 1, or 2 following the shot.
Serious Injuries 230,364
Hospitalizations 110,600
Miscarriages 2,887
Permanently Disabled 35,650
Breakthrough COVID-19 – 53% higher risk of death, 59% higher risk of at least one new medical condition – lungs, other organs. Data from VA: 16,035 survivors of breakthrough infections, 48,536 unvaccinated COVID-19 survivors, 3.6 M uninfected (Research Square)
CLINICAL TRIALS
CLINICAL TRIALS for these shots lasted only a few months, had samples that did not represent the total population, had poor predictive power for adolescents/children because of their small size, participants not monitored after injection, no timely follow-up of patients who experienced adverse events, protocol deviations not reported, vaccines not stored at proper temperatures, and mislabeled specimens. And importantly, the clinical trials did not address long-term effects that, if serious, children/adolescents would be subjected to for decades.
Toby Rogers Ph.D., whose focus is on corruption in the pharmaceutical industry, wrote on October 25, 2021: Ten red flags in the FDA’s risk-benefit analysis of Pfizer’s EUA application to inject American children 5 to 11 with its mRNA product. This section is taken directly from Dr Roger’s report.
“The FDA’s risk-benefit analysis in connection with Pfizer’s Emergency Use Authorization (EUA) application to inject children ages 5 to 11 with their COVID-19 vaccine is one of the shoddiest documents I’ve ever seen.
1 • COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750). So any claims you see in the press about the Pfizer vaccine being “90% effective” in children are meaningless because they are referring to mild cases from which children usually recover quickly (and then have robust broad spectrum immunity). So there is literally no emergency in this population for which one could apply for Emergency Use Authorization. Pfizer’s application should be dead on arrival if the FDA actually followed the science and their own rules.
2 • Pfizer’s clinical trial in kids was intentionally undersized to hide harms. This is a well known trick of the pharmaceutical industry. The FDA even called them out on it earlier this summer and asked Pfizer to expand the trial and Pfizer just ignored them because they can. (Pfizer fudged it by importing data from a different study but this other study only monitored adverse outcomes for 17 days so if anything the new data polluted rather than clarified outcomes). To put it simply, if the rate of particular adverse outcome in kids as a result of this shot is 1 in 5,000 and the trial only enrolls 1,518 in the treatment group then one is unlikely to spot this particular harm in the clinical trial. Voilà “Safe & Effective.”
3 • Pfizer only enrolled “participants 5-11 years of age without evidence of prior SARS-CoV-2 infection.” Does the Pfizer mRNA shot wipe out natural immunity and leave one worse-off than doing nothing as shown in this data from the British government? Pfizer has no idea because children with prior SARS-CoV-2 infection were excluded from this trial. This was by design. Toxic polluters have learned to not ask questions that they do not want the answers to, lest they wind up staring at their own smoking gun in a future court case.
According to an analysis by Alex Berenson:
‘What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus. Specifically, vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people. This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably). It also means the virus is likely to select for mutations that go in exactly that direction because those will essentially give it an enormous vulnerable population to infect. And it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.’
4 • Did Pfizer LOSE CONTACT with 4.9% of their clinical trial participants? The FDA risk-benefit document states: “Among Cohort 1 participants, 95.1% had safety follow-up ≥2 months after Dose 2 at the time of the September 6, 2021 data cutoff.” So what happened with those 4.9% who did not have safety follow-up 2 months after Dose 2? Were they in the treatment or control group? We have no idea because Pfizer isn’t saying. Given the small size of the trial, failing to follow up with 4.9% of the participants potentially skews the results.
5 • The follow up period was intentionally too short. This is another well-know trick of the pharmaceutical industry designed to hide harms. Cohort 1 appears to have been followed for 2 months, cohort 2 was only monitored for adverse events for 17 days. Many harms from vaccines including cancer and autoimmune disorders take much longer to show up.
6 • The risk-benefit model created by the FDA only looks at one known harm from the Pfizer mRNA shot — myocarditis. But we know that the real world harms from the Pfizer mRNA shot go well beyond myocarditis and include anaphylaxis, Bell’s Palsy, heart attack, thrombocytopenia/ low platelet, permanent disability, shingles, and Guillain-Barré Syndrome (GBS) to name a few. Cancer, diabetes, endocrine disruption, and autoimmune disorders may show up later. But the FDA does not care about any of that because they have a vaccine to sell so they just ignore all of those factors in their model.
7 • Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo. They claim that they are doing this for “ethical reasons”. But everyone knows that Pfizer’s true aim is to wipe out any comparison group so that there can be no long term safety studies. Wiping out the control group is a criminal act and yet Pfizer, Moderna, J&J, and AZ do this as standard practice with the blessing of the FDA/CDC.
8 • Given all of the above, how on earth did the FDA claim any benefits at all from this shot? You should probably sit down for this part because it’s a doozy! Here’s the key sentence:
Vaccine effectiveness was inferred by immunobridging SARS-CoV-2 50% neutralizing antibody titers (NT50, SARS-CoV-2 mNG microneutralization assay).
Wait, what!? I’ll explain. There were ZERO cases of severe COVID-19 in the clinical trial of children ages 5 to 11. So Pfizer and the FDA just ignored all of the actual health outcomes (they had to, there is no emergency, so the application is moot). INSTEAD Pfizer switched to looking at antibodies in the blood. In general, antibodies are a poor predictor of immunity. And the antibodies in the blood of these 5 to 11 year old children tell us nothing because again, there were zero cases of severe COVID-19 in this study (none in the treatment group, none in the control group). So Pfizer had to get creative! What they came up with is “immuno-bridging”. Pfizer looked at the level of antibodies in the bloodwork of another study, this one involving people 16 to 25 years old, figured out the level of antibodies that seems to be protective in that population, then figured out how many kids ages 5 to 11 had similar levels of antibodies in their blood, and then came up with a number for how many cases, hospitalizations, ICU admissions, and deaths would be prevented by this shot in the 5 to 11 population in the future, based on the antibody levels and health outcomes from the 16 to 25 year old population. If your head hurts from that tortured logic, it should, because such chicanery is unprecedented in a risk-benefit analysis.
So when the FDA uses this tortured logic at the beginning of their briefing document, all of the calculations that stem from this will be flat out wrong. Not just wrong but preposterous and criminally wrong.
The whole ballgame comes down to Table 14 on page 34 of the FDA’s risk-benefit document. And there the red flags come fast and furious.
9 • The FDA model only assesses the benefits of vaccine protection in a 6-month period after completion of two doses. Furthermore it assumes constant vaccine efficacy during that time period. This is problematic on several counts.
First, reducing mild cases in children is not a desired clinical outcome. As Dr. Geert Vanden Bossche points out, mass vaccination turns kids into shedders of more infectious variants.
‘Under no circumstances should young and healthy people be vaccinated as it will only erode their protective innate immunity towards Coronaviruses (CoV) and other respiratory viruses. Their innate immunity normally/ naturally largely protects them and provides a kind of herd immunity in that it dilutes infectious CoV pressure at the level of the population, whereas mass vaccination turns them into shedders of more infectious variants. Children/ youngsters who get the disease mostly develop mild to moderate disease and as a result continue to contribute to herd immunity by developing broad and long-lived immunity. If you are vaccinated and get the disease, you may develop life-long immunity too but why would you take the risk of getting vaccinated, especially when you’re young and healthy? Firstly, there is the risk of potential side effects; secondarily, there is the ever increasing risk that your vaccinal antibodies will no longer be functional while still binding to the virus, thereby increasing the likelihood of ADE or even severe disease….’
Second, we know that vaccine efficacy in the month after the first dose is negative because it suppresses the immune system and it begins to wane after 4 months so all of the FDA’s estimates of vaccine efficacy are inflated.
Third, the harms of myocarditis from these shots will likely unfold over the course of years. Robert Malone, the inventor of mRNA technology notes that the FDA is admitting that children will be injected twice a year forever (hence the six month time frame in the FDA risk-benefit model). But the risks of “adverse events such as cardiomyopathy will be cumulative.” So any model that only looks at a six month time frame is hiding the true adverse event rate.
10 • The FDA/Pfizer play fast and loose with their estimates of myocarditis. First they estimate “excess” (read: caused by the shot) myocarditis using data from the private “Optum health claim database” instead of the public VAERS system (p. 32). So it’s impossible for the public to verify their claims. Then, when it comes to estimating how many children with vaccine-induced myocarditis will be hospitalized and admitted to the ICU they use the Vaccine Safety Datalink (see page 33). Why switch to a different database for those estimates? Finally, there is no explanation for how they calculated “excess” myocarditis deaths, so they just put 0. Red flag, red flag, red flag.
The FDA estimates that there will be 106 extra myocarditis cases per 1 million double-jabbed children 5-11. There are 28,384,878 children ages 5 to 11 in the U.S. The Biden administration wants to inject Pfizer mRNA shots into all of them and has already purchased enough doses to do just that (even though only 1/3rd of parents want to jab their kids with this shot). So (if the Biden administration has its way) 106 excess myocarditis cases per 1 million x 28.38 million people would be 3,009 excess myocarditis cases post-vaccination if the Pfizer vaccine is approved.
And over the course of several years many of those children will die. Dr. Anthony Hinton (“Consultant Surgeon with 30 years experience in the NHS”) points out that myocarditis has a 20% fatality rate after 2 years and a 50% fatality rate after 5 years. So the FDA has it exactly backwards — they want to prevent mild COVID in children which reduces herd immunity and they just flat out lie about the harms from myocarditis.
I’ve taken the liberty to correct the FDA’s Table 14 with actual real world data and extended it over 5 years. It looks like this:
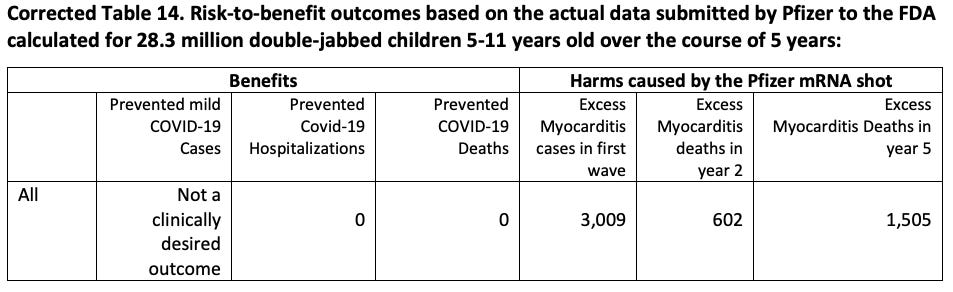
A study by Harvard Pilgrim Healthcare for the U.S. Department of Health and Human Services estimated that VAERS only captured 1% of actual vaccine injuries. Steve Kirsch has done elaborate modeling that puts the Under-Reporting Factor of COVID-19 vaccine deaths at 41 (so multiply the above numbers by 41). And myocarditis is just one of a multitude of possible harms from COVID-19 vaccines. Dr. Jessica Rose recently calculated an Under-Reporting Factor of 31 for all severe adverse events following vaccination.
Conclusion by Toby Rogers, Ph.D.
The Pfizer vaccine fails any honest risk-benefit assessment in connection with its use in children ages 5 to 11. The FDA’s risk-benefit analysis of Pfizer’s mRNA vaccine in children ages 5 to 11 is shoddy. It used tortured logic (that would be rejected by any proper academic journal) in order to reach a predetermined result that is not based in science. The FDA briefing document is a work of fiction and it must be withdrawn immediately. If the FDA continues with this grotesque charade it will cause irreparable harms to children and the FDA leadership will one day be prosecuted for crimes against humanity.”
RELATIVE vs ABSOLUTE RISK REDUCTION
Pfizer reported that its vaccine shows a 95% efficacy. That sounds like it protects you 95% of the time. But that’s not what that number actually means. That is the relative risk reduction which does NOT tell you what your overall risk is reduced by vaccination. For that number, we need to look at absolute risk reduction. This video explains the difference and why it’s important to understand.
https://rumble.com/vobcg5-relative-vs-absolute-risk-reduction.html
SPIKE PROTEINS and LIPID NANOPARTICLES CAUSE HARM
Spike proteins from Covid-19 infection and/or spike proteins made from the shots can cause inflammation and organ dysfunction when they bind to the ACE2 docking sites on human cells of the Mucus Membranes, Eye, Respiratory Tract, Heart / Blood Vessels, Brain, Musculoskeletal, Reproductive organs, Gastrointestinal, Kidney, Skin. This binding to organs occurs before antibodies are made to the spike proteins.
The shots cause the recipient to create trillions of spike proteins for an unknown period of time.
(https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8437699/)
The part of the spike protein that docks on the human ACE2 receptor is called the S1 segment. This S1 is found in human white cells (monocytes) for up to 15 months after infection – this explains the long haul syndrome. This S1 is also found in monocytes of those who have been vaccinated for at least the same length of time – the study was not continued after 15 months.
Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) Up to 15 Months Post-Infection https://www.biorxiv.org/content/10.1101/2021.06.25.449905v3
Severe Acute Respiratory Syndrome Coronavirus 2 Spike Protein Based Novel Epitopes Induce Potent Immune Responses in vivo and Inhibit Viral Replication in vitrohttps://pubmed.ncbi.nlm.nih.gov/33841395/
The SPIKE PROTEINS:
(1) do not remain in the local shoulder injection but travel in the blood to virtually all organs of the body.
(2) can cause disease by attaching and damaging endothelial, lung, heart, brain, musculoskeletal, gastrointestinal, reproductive organs, kidney, skin cells, forming clots and inhibiting mitochondria – raising serious long-term concerns.
(3) interact in many signaling pathways which may initiate cancers and other serious diseases.
(4) could cause autoimmunity in susceptible subgroups, and could exacerbate autoimmunity for those who already have autoimmune diseases – based on the finding that anti-SARS-CoV-2 protein antibodies cross-reacted with 28 of 55 diverse human tissue antigen, and Antibody-Dependent Enhancement.
Thousands of LIPID NANOPARTICLES (LNP) encapsulate the mRNA of the shot and these are highly inflammatory.
The labels for Comirnaty and BioNtech state that the vaccination should not be given to individuals who are allergic to ingredients. One ingredient is Polyethylene glycol (PEG) which is similar to Propylene Glycol, an ingredient in antifreeze. Polyethylene glycol (PEG) is an adjuvant which causes an immune response without carrying any vaccine at all. About 72% of the population already have PEG antibodies that may cause severe anaphylactic response requiring hospitalization or death, or life-long allergies and anti-drug antibodies (ADAs) which could stop other medications from working in your body. Another ingredient of the Lipid Nanoparticle delivery system is “ALC 0315” in the Pfizer shots. The Safety Data Sheet for this primary ingredient states that it is Category 2 under the OSHA HCS regulations (21 CFR 1910) and includes several concerning warnings. Since these vaccines often require a booster shot, anti-PEG antibody formation is expected after the first shot. Thus, the allergic events are likely to increase with each shot.”
Do we have all the information we need? Of course not. On November 18, 2021 the FDA asked a federal judge not to fully release Pfizer vaccine data until the year 2076: 500 pages/month of the 329,000 pages – that’s 20,000 days. FDA was nimbly able to review and issue license in 108 days.
Pfizer has no liability, got billions and we can’t see the data.
By injecting the mRNA “vaccine” as opposed to a natural infection, a young body is flooded with a large volume of spike protein and the toxic encapsulating LNP layer thus bypassing the body’s protective innate immune system.
PFIZER VACCINE ENTERS LIVER CELLS AND GETS CONVERTED TO DNA
According to Swedish researchers at Lund University, the messenger RNA (mRNA) from Pfizer’s COVID-19 vaccine is able to enter human liver cells and is converted into DNA. In the human liver cell’s nucleus, the mRNA vaccine initiates the cell’s DNA to produce LINE-1 gene to make mRNA. That mRNA leaves the nucleus, enters the cell’s cytoplasm and translates into LINE-1 protein. A portion of this protein (open reading frame-1 or ORF-1) goes back into the nucleus where it attaches to the vaccine’s mRNA and reverse transcribes into spike DNA. The normal transcription process involves a portion of the DNA serving as a template to make an mRNA molecule inside the nucleus. The CDC said this conversion would never happen.
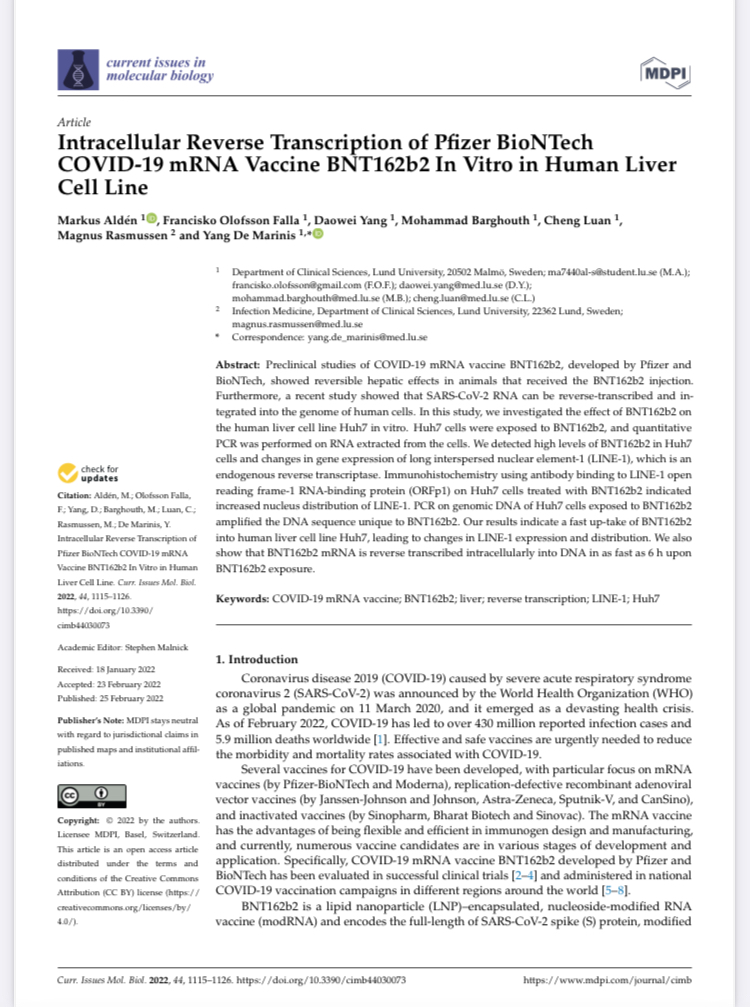
https://www.mdpi.com/1467-3045/44/3/73/htm#B39-cimb-44-00073 file:///C:/Users/chuck/Downloads/cimb-44-00073.pdf
A person may experience any of the following:
Mucus membranes: Running nose, sneezing, burning and itchy eyes.
Respiratory Tract: shortness of breath, congestion, pneumonia, persistent cough, etc.
Heart / Blood Vessels: myocarditis, heart attack, pericarditis, chest pain, arrhythmias, blood pressure changes, blood clotting, etc.
The spike protein attaches to the sialic acid residues of red blood cells, causing red cell clumping and starts the coagulation cascade. Routine blood tests to detect clotting, like D-dimer, may or may not be elevated.
Most individuals with myocarditis do not have any symptoms. Complications of myocarditis include dilated cardiomyopathy, arrhythmias, sudden cardiac death and carries a mortality rate of 20% at one year and 50% at 5 years. According to the National Center for Biotechnology Information, U.S. National Library of Medicine, “despite optimal medical management, overall mortality has not changed in the last 30 years.” COVID 19 can cause heart attack, myocarditis, abnormal QRS axis in 20%, conduction abnormalities in 20%, premature beats in 10%, atrioventricular block in 2.5%, ST and T wave changes, 9.3% have arrhythmias, mostly atrial fibrillation.
mRNA COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and Acute Coronary Syndrome Risk as Measured by the PULS Cardiac Test. “We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.” https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.10712
Because heart inflammation occurs in young people in the very short term the FDA added a warning label to the Pfizer and Moderna vaccines about myocarditis and pericarditis.
VIRAL MYOCARDITIS RESULTS IN 2 IN 10 PEOPLE DEAD AFTER 2 YEARS AND 5 IN 10 AFTER 5 YEARS.
ACUTE CARDIAC INJURY AND NORMALIZATION OF TROPONIN AFTER HOSPITAL
“There were 4,248 (39.7%) COVID-19 patients with ACUTE CARDIC INJURY (ACI) and most (93%) developed ACI on or within a day after admission. In-hospital mortality of ACI patients was high compared to non-ACI patients. Of the 2,880 ACI survivors, 1,114 (38.7%) returned to the hospital 2.5 months on average post-discharge, of which only 302 (44.9%) out of 673 patients recovered from ACI. There were no significant differences in demographics, race, ethnicity, major commodities, and length of hospital stay between groups. Prediction of ACI recovery post-discharge using the top predictors (troponin, creatinine, lymphocyte, sodium, lactate dehydrogenase, lymphocytes and hematocrit) at discharge yielded 63.73%-75.73% accuracy.”
Persistent cardiac injury is common among COVID-19 survivors. Readily available patient data accurately predict ACI recovery post-discharge.
https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(22)00010-X/fulltext?fbclid=IwAR1w1Z1_tdQ25kBW4TS3qIn5EeS8hJej58H1sTZ2qoGCejFaefwG77dE-xQ
Increased Heart Disease, Stroke Risk After Surviving Even Mild Covid-19
U.S. veterans who had survived even mild Covid-19 infections were 63% more likely to have a greater risk of cardiovascular problem in the ensuing year: 52% stroke, 63% heart attack, 72% heart failure, 71% atrial fibrillation, 84% sinus tachycardia, 53% sinus bradycardia, and 84% ventricular arrhythmias.

https://www.nature.com/articles/s41591-022-01689-3%20
Brain: ‘Leaky’ Blood-Brain Barrier (BBB), brain fog or difficulty concentrating, loss of smell, malaise, fatigue, headaches or migraines that come on suddenly become worse with standing and get more severe as the day progresses, depression, insomnia, vertigo, panic attacks, tinnitus, etc. ADD / ADHD / Autism spectrum disorders. If the BBB is damaged or weakened in some way, immune cells are able to cross and attack the myelin around your nerves, which leads to nerve damage and MS symptoms.
Babies born to mothers who suffered COVID-19 disease during pregnancy seem to exhibit differences in neurodevelopmental outcomes at 6 weeks, according to a preliminary analysis presented in the 30th European Congress of Psychiatry. https://medicalxpress.com/news/2022-06-babies-exposed-covid-womb-neurodevelopmental.html?fbclid=IwAR1A6r71ndKRWyxeV4Y_ZgubpyCNe8hwBQ6LybsBvnGTdmcEmiwpWuxA12U
Musculoskeletal: muscle and joint pain, chronic fatigue that does not improve with rest, weakness, inability to exercise, unable to perform normal activities.
Gastrointestinal: Anorexia, diarrhea, bloating, vomiting, nausea, etc.
Skin: Itching, rashes, hair loss.
Reproductive: 30,000+ Women in UK Report Menstrual Problems After COVID Shots, But Menstrual Issues Not Listed as Side Effect. Also, still births and abortions are reported after the shot.
Cancer: Higher risk because the spike also binds to and renders the p53 gene ineffective. The p53 gene is a cancer suppressor gene that stops the formation of cancers.
A natural COVID-19 infection provides both systemic protection (IgG antibodies and cellular activation) as well as protection in the nasal passages and respiratory tree (IgA antibodies). The shots do not provoke IgA antibody production and therefore do not provide protection in the nasal passages and respiratory tree. That is why there are so many cases of breakthrough infections in those who have been fully vaccinated and that is why fully vaccinated people can harbor the virus in their nasal passages that can potentially be spread to others.
Children’s innate immunity, the low number of ACE2 receptors, and some other factors protect them and provides a kind of herd immunity. Mass vaccination, on the other hand, makes them shed more infectious variants. And when children get infected they have mild to moderate disease with durable immunity that contributes to herd immunity.
The COVID-19 reported deaths are people who died with COVID-19, not necessarily from COVID-19 – 94% of the deaths had multiple comorbidities as reported by the CDC. There are high false positives from the high amplification cycle PCR tests. And some healthcare professionals are willing to attribute death to COVID-19 in the absence of tests or sometimes even with negative PCR tests. Together these greatly reduce the CDC’s numbers attributed to COVID-19 for all age groups.
By injecting the mRNA shots as opposed to a natural infection, a child is flooded with a large volume of spike protein and the toxic encapsulating LNP layer thus bypassing the body’s protective innate immune system.
The MANDATES
On November 12, 2021, the 5th Circuit Court of Appeals in New Orleans Struck down Biden vaccine Mandate. And despite that, the White House tells businesses to move forward with the Biden mandates.
Secretary of Defense Austin ordered Covid Vaccine mandates: “Unit personnel should use only as much force as necessary to assist medical personnel with immunizations.” Use of force to give treatment against the will of a mentally competent person is medical battery & violates ethics.
Ensuring the health of the fighting force is a strategic imperative, for which every military physician is responsible to ensure. This “vaccine” represents a risk for young males.
Aircrew Training Program (ATP) 5-19, 1-8. Accept No Unnecessary Risk, states, “An unnecessary risk is any risk that, if taken, will not contribute meaningfully to mission accomplishment or will needlessly endanger lives or resources. Army leaders accept only a level of risk in which the potential benefit outweighs the potential loss.
And worse of all is what the World Health Organization states:
“the [mere] presence of a child in the classroom at the vaccination session implies consent” for the shot
Who influences W.H.O.?
Who is the largest contributor to W.H.O.?

FACIAL MASKS ARE NOT VERY EFFECTIVE
Watch at time marker 3:00:50to 3:08:30 from Full Hearing: COVID-19: A Second Opinion Hosted By Sen. Ron Johnson.
Charles B. Simone M.MS., M.D. Conclusion:
Based on hundreds of medical studies, the real risk for healthy children is about zero. And they have a very low risk of getting infected or spreading an infection to other children or adults. Therefore any mandates or mass injections or even clinical trials is unjustified, unethical and potentially associated with a significant lifetime of disability and even death. Above All Do No Harm.
COVID-19 BIOWEAPON² PART 1 Executive Summary https://bit.ly/3Fuiwdu
Written: March 2020
BIOWEAPON 1 – virus
BIOWEAPON 2 – shots
COVID-19 BIOWEAPON² PART 2 https://bit.ly/3eI11bK
COVID-19 BIOWEAPON² PREREQUISITE FOR U.S. INVASION – LONG TERM PLANNING
https://tinyurl.com/37fbrevd
COUNTERMEASURE “VACCINE” – NOT EFFECTIVE, NOT SAFE, NOT MADE AT “WARP SPEED”
https://tinyurl.com/5n7tajc5
CHILDREN SHOULD NOT GET THE “VACCINE”
“ABOVE ALL DO NO HARM”
Written November 21, 2021 https://bit.ly/3nB4CyK
PROTECT YOURSELF FROM THE SPIKE: COVID-19 INFECTION and/or VACCINE – OUR NEXT HEALTH CRISIS
Written August 23, 2021 https://bit.ly/3kkrejY

