

Updated March, 2021
We do not diagnose disease or recommend a dietary supplement for the treatment of disease. You should share this information with your physician who can determine what nutrition, disease and injury treatment regimen is best for you. You can search this site or the web for topics of interest that I may have written (use Dr Simone and topic).
“We provide truthful information without emotion or influence from the medical establishment, pharmaceutical industry, national organizations, special interest groups or government agencies.” Charles B Simone, M.MS., M.D.
ASPIRIN – WHAT DOSE, WHAT FORM, WHEN TO TAKE IT, BENEFIT
https://bit.ly/3s3yZ0x
Lawrenceville, NJ (Dr Simone) – Despite aspirin’s very short half life of only 15-20 minutes, it causes permanent and irreversible changes to platelets and other factors when taken daily. A non-coated 325 mg aspirin taken at around 6 PM is effective at reducing the risk of heart attack, stroke, other cardiovascular events, and cancer.
But there are multiple reasons why aspirin treatment fails (1-7):
1) patients don’t take it routinely;
2) non-steroidal anti-inflammatory drugs interfere with aspirin;
3) diabetics have a higher production of platelets;
4) enteric coating reduces bioavailability; and,
5) a person’s weight more than 154 lb (70 kg)
WHAT DOSE – 325 mg
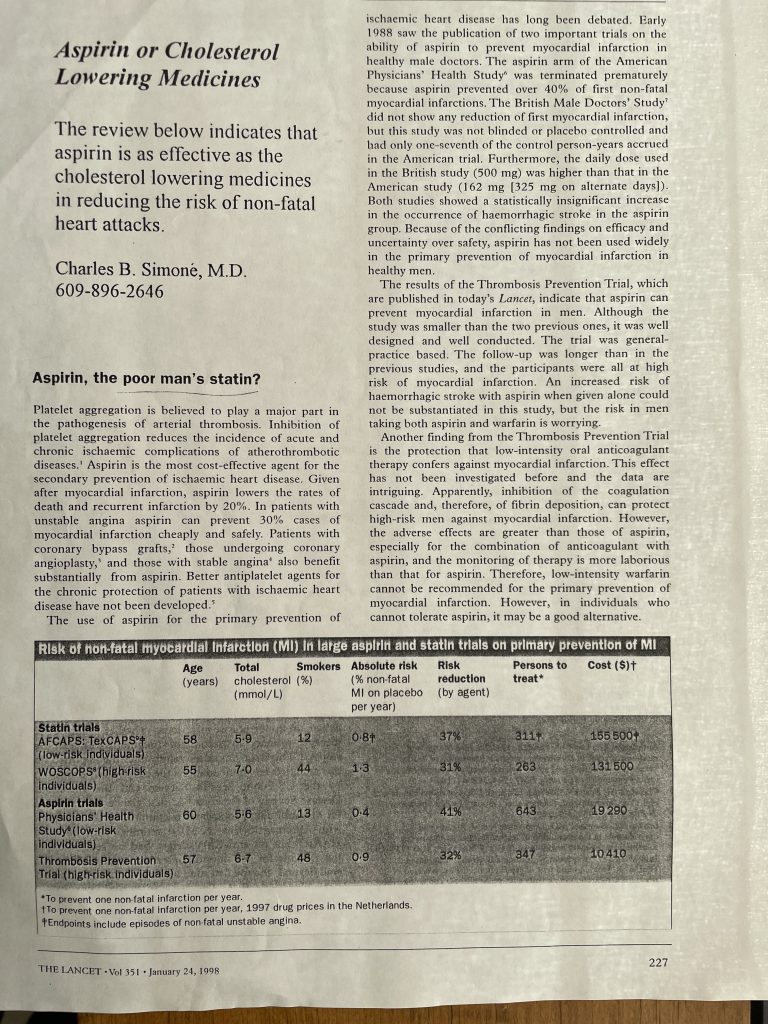
81 mg per day “baby aspirin” has an anti-platelet effect because it inhibits an enzyme, COX-1 [cyclooxygenase-1]. Platelets initiate clotting. Low dose aspirin (75-100 mg per day) was only effective in preventing vascular events for patients weighing less than 154 lb (70 kg) and had no benefit in 80% of men and 50% of women weighing more than 154 lb (70 kg).
325 mg per day inhibits COX-1 and COX-2 resulting in anti-platelet effects as well as anti-inflammatory and anti-pain effects.
325 mg aspirin is effective for those weighing more than 154 lb (70 kg).
325 mg aspirin is an anticoagulant because it inhibits thromboxane A2, reduces inflammatory cytokines, oxygen radicals, and growth factors.
325 mg aspirin inhibits thromboxane A2 much more rapidly than 81 mg and therefore acts more quickly as an anticoagulant.
Thromboxane A2 is a potent vasoconstrictor and promoter of platelet aggregation.
Aspirin is also an antiangiogenic agent, interfering with blood vessel formation and thereby interrupts the blood supply to feed cancers.
WHAT FORM – non-coated aspirin
Aspirin is rapidly absorbed with a bioavailabilty of about 50%, but much lower when given as the enteric coated form. Peak concentration of non-coated aspirin occurs rapidly within 30 minutes after ingestion but up to 4 hours after ingesting enteric coated aspirin. Rapid peak concentration is desirable and therefore you need to use non-enteric coated aspirin. Take non-coated aspirin with food. Food will act as the buffer. Most stores sell only the enteric coated aspirin. So you will have to search for the non-coated aspirin – try a dollar store.
WHEN TO TAKE IT – 6 PM
You have a system in your body that breaks down blood clots called the fibrinolytic system. It has a circadian rhythm peaking at 6 PM with its lowest level of activity at 6 AM. We are unprotected in the early hours of the morning – in fact, most heart attacks and strokes occur between 3 AM and 5 AM. Therefore, take your non-coated 325 mg aspirin at around 6 PM with your large meal so that you have protection throughout the night.
BENEFIT
-
Decreases the risk for heart attach and stroke – 325 mg aspirin. The magnitude and benefits of aspirin in preventing early TIA and recurrent ischemic stroke are greater than previously recognized ( Stroke. Lancet. 2017. 389:641-54) and also an earlier Lancet article published January 24, 1998 (below).
-
-
Decreases Lipoprotein (a)
LIPOPROTEIN (a) is LOWERED BY NIACIN, ASPIRIN, and VITAMIN C
NIACIN – NICOTINIC ACID FORM – LOWERS CHOLESTEROL, LDL, TRIGLYCERIDES, AND RAISES HDL -
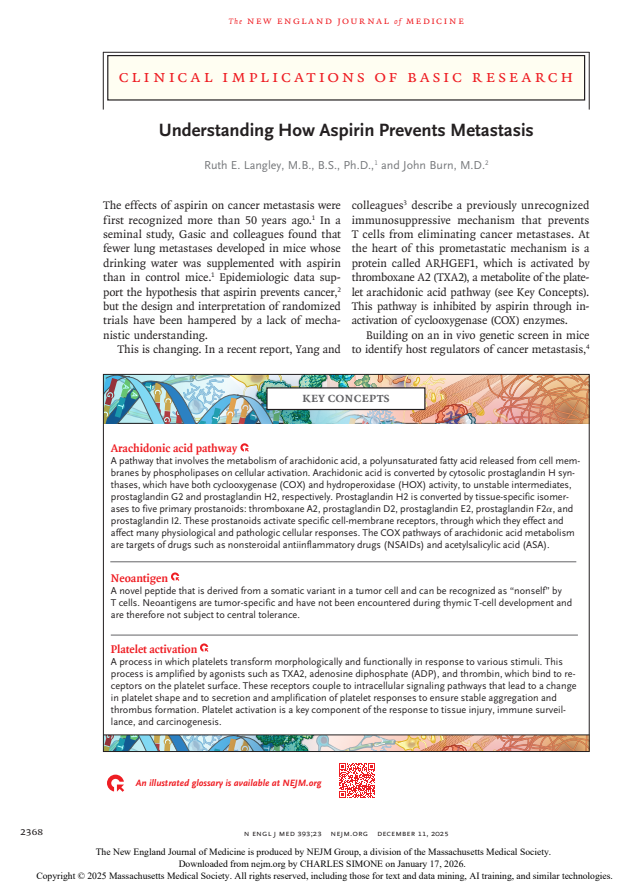
Decreases the risk for cancer (8), especially colon cancer and colon polyps (9). Long-term aspirin use was associated with a modest but significantly reduced risk for overall cancer, especially gastrointestinal tract tumors. Regular aspirin use may prevent a substantial proportion of colorectal cancers and complement the benefits of screening. Low dose aspirin is not effective for those who weigh more than 154 lb (70 kg).
-
Aspirin Use Is Associated With Decreased Mechanical Ventilation (44% reduction), Intensive Care Unit Admission (43% reduction), and In-Hospital Mortality (47% reduction) for COVID-19 patients.There were no differences in major bleeding or overt thrombosis between aspirin users and non-aspirin users (10). The dose used in this study was 81 mg.
-
Aspirin Prevents Colorectal Cancer in patients with Lynch Syndrome, an inherited disease that increases the risk of colorectal cancer.
References
1. Hennekens CH, Schneider WR, Herbert PR, Tantry US, Gurbel, PA. Hypothesis formulation from subgroup analyses: nonadherence or nonsteroidal anti-inflammatory drug use explains the lack of clinical benefit of aspirin on first myocardial infarction attributed to “aspirin resistance.” Am Heart J. 2010 May;159(5):744-8
2. Li X, Fries S, Li R, Lawson JA, Propert KJ, Diamond SL, Blair IA, FitzGerald GA, Grosser T. Differential impairment of aspirin-dependent platelet cyclooxygenase acetylation by nonsteroidal anti-inflammatory drugs. Proc Natl Acad Sci USA. 2014 Nov 25;111(47):16830-5.
3. Rothwell PM, Cook NR, Gaziano JM, Price JF, Belch JFF, Roncagliani MC, Morimoto T, Mehta Z. Effects of aspirin on risks of vascular events and cancer according to bodyweight and dose: analysis of individual patient data from randomized trials. Lancet. 2018; 392:387-99. Lancet. 2018 Aug 4;392(10145):387-399. doi: 10.1016/S0140-6736(18)31133-4. Epub 2018 Jul 17.
4. Pascale S, Petrucci G, Dragani A, Habib A, Zaccardi F, Pagliaccia F, Pocaterra D, Ragazzoni E, Rolandi G, Rocca B, Patrono C. Aspirin-insensitive thromboxane biosynthesis in essential thrombocythemia is explained by accelerated renewal of the drug target. Blood. 2012 Apr 12;119(15):3595-603.
5. Maree AO, Curtin RJ, Dooley M, et al. Platelet response to low-dose enteric-coated aspirin in patients with stable cardiovascular disease. J Am Coll Cardiol. 2005; 46:1258-63.
6. Grosser T, Fries S, Lawson JA, Kapoor SC, Grant Gr, FitzGerald GA. Drug resistance and pseudoresistance: an unintended consequence of enteric coating aspirin. Circulation. 2013; 127:377-85.
7. Patrono C. Aspirin. Chapter 53. Platelets. Academic Press. 2013. Pages 1099-1115.
8. https://www.nejm.org/doi/pdf/10.1056/NEJMcibr2502386
9.
Anesthesia & Analgesia: April 2021 – Volume 132 – Issue 4 – p 930-941 doi: 10.1213/ANE.0000000000005292

