

We do not diagnose disease or recommend a dietary supplement for the treatment of disease. You should share this information with your physician who can determine what nutrition, disease and injury treatment regimen is best for you. You can search this site or the web for topics of interest that I may have written (use Dr Simone and topic).
“We provide truthful information without emotion or influence from the medical establishment, pharmaceutical industry, national organizations, special interest groups or government agencies.” Charles B Simone, M.MS., M.D.
CORONAVIRUS FLU COVID-19
https://bit.ly/2w8Hr6C
Lawrenceville, NJ (Dr Charles Simone) – –
Feb 14, 2021 – People who have COVID-19 disease and are obese or are older exhale three times more respiratory droplets that spread the infection. This occurs even among those with asymptomatic cases of COVID-19 (Proceedings Natl Acad Sci https://doi.org/10.1073/pnas.2021830118).
June 3, 2020 – Lancet and New England Journal of Medicine Published Flawed Studies
Lancet and New England Journal of Medicine Published Flawed Studies about Covid-19 patients indicating that certain heart medicines (ACE inhibitors and ARBs) are safe and that hydroxychloroquine is not safe. These conclusions are erroneous.
The data for these articles were supplied by Surgisphere, a little known health analytics company with 3 employees who have little or no scientific background – one is an adult model/events hostess, one is a science fiction author, and the third is the chief executive, Sapan Desai, who is a co-author on both studies. Surgisphere has fewer than 170 followers on Twitter with no posts between October 2017 and March 2020. This should have raised a red flag for both journals but it did not. Both journals issued an “Expression of Concern” pending investigation. Finally, both articles were retracted on June 6, 2020.
On May 1, 2020 the New England Journal of Medicine published a peer-reviewed study involving 8900 patients with Covid-19 in 169 hospitals in Asia, Europe, and North American showing no increased risk of in-hospital death with the use of ACE inhibitors or ARBs.
On May 22, 2020 the Lancet published a peer-reviewed study of 96,000 patients with Covid-19, admitted to 671 hospitals around the world showing hydroxychloroquine caused a higher death rate and increased heart problems. Because of these negative findings, the World Health Organization stopped their hydroxchloroquine study.
Big red flag: How could a three person company gather all that data in a few weeks from around the world involving tens of thousands of patients from 840 hospitals with different languages and coding systems, regulatory and ethical practices of every country? This alone should have prevented these peer-reviewed prestigious journals from even looking at these papers, let alone publishing them; not to mention the other authors who put their names on the papers just to have another paper on their curriculum vitae.
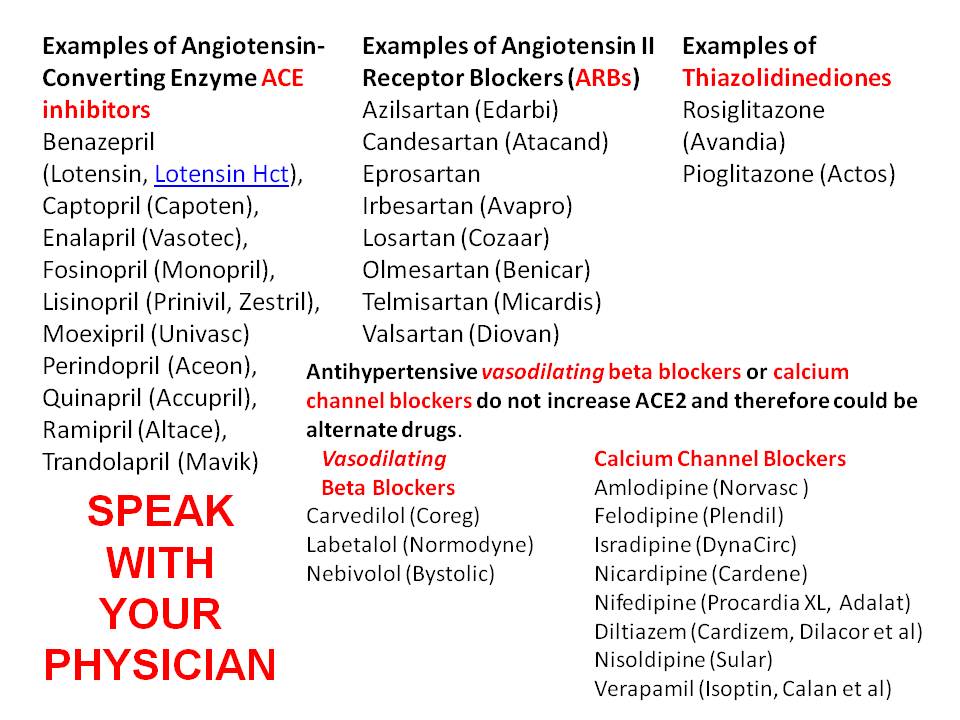
I have written that patients should speak with their physician about switching from an ACE inhibitor or ARB to a vasodilating beta blocker and/or calcium channel blocker to control their blood pressure because ACE inhibitors and ARBs increase the Covid-19 receptors on human cells and thereby allow infection.
DRUGS INCREASE RISK FOR SARS-CoV-2 (COVID-19) INFECTION https://bit.ly/2J1YJW6
And the Center for Disease Control and Prevention published a paper entitled “Chloroquine is a potent inhibitor of SARS coronavirus infection and spread.”
COVID-19 BIOWEAPON https://bit.ly/3eI11bK
May 7, 2020 – 66% of New York state coronavirus hospitalizations are people staying at HOME and NOT essential workers – which begs question: Does lockdown even work? (DailyMail.com)

April 10, 2020 SARS-Cov-2 (COVID-19) HAS MUTATED 160 TIMES
Coronaviruses are RNA viruses and mutate often when they replicate quickly. A vaccine is made to a specific strain and therefore will be progressively less effective with each succeeding mutation of the virus.
Phylogenetic network analysis of SARS-CoV-2 genomes – phylogenetic network of 160 largely complete SARS-Cov-2
genomes://www.pnas.org/content/pnas/early/2020/04/07/2004999117.full.pdf?fbclid=IwAR1Z6W96w_-U5UZ9NtFkiddWPEmZTC1FXDwmFGK-xslIvRKQGzruzPjvCyA
April 9, 2020 ARE VENTILATORS OVERUSED?
Some critical care physicians say that putting coronavirus patients on ventilators could be of little benefit to many and even harmful to some because their breathing muscles work well without the need for high pressure mechanical ventilation that can harm lungs. These coronavirus patients have extremely low blood oxygen levels but do not gasp for air, or have fast heart rates, or brain dysfunction. Therefore, some of these patients could be treated with noninvasive respiratory support like nasal cannula, or breathing masks used for sleep apnea (CPAP) or bilevel positive airway pressure ventilators (BiPAP). Oxygen is delivered through the nose, or via a tube into a face mask without the need for intubation and sedation.
Usually the decision to put patients on a ventilator is the level of blood oxygen. Physicians have been intubating these patients when their blood oxygen levels are in their 70s or lower. The Chinese have indicated that early intubation will save critical organs and patients from dying. But Greg Martin, a critical care physician at Emory University School of Medicine and president-elect of the Society of Critical Care Medicine said that most hospitals are using simpler, noninvasive strategies first – nasal cannulas (two-prongs in the nose), CPAP, and BiPAP. Then a ventilator is used if the oxygen level is too low or the oxygen level does not respond, and/or if the patient’s breathing muscles get too weak.
A critical care physician, Dr Cameron Kyle-Sidell at a New York City hospital has said that because U.S. physicians had never seen Covid-19 before February, they are basing clinical decisions on conditions that may not be good guides. This may be an entirely new disease making ventilator protocols developed for other conditions less than ideal.
April 8, 2020 HYPERTENSION AND DIABETES ARE THE LEADING COMORBIDITIES AMONG COVID-19 DEATHS IN NEW YORK
SPEAK WITH YOUR DOCTOR ABOUT YOUR DRUGS THAT MAY INCREASE YOUR RISK FOR COVID-19.
The Cardiology Societies should re-examine their opinion.
March 5, 2020 COVID-19 HAS ALREADY MUTATED
According to scientists in China and published in the National Science Review, coronavirus COVID-19 in China after only a few months has already mutated to a second strain. The two strains are the S type (30%) and the more aggressive L type (70%). Coronaviruses are RNA viruses and mutate often when they replicate quickly. When I was interviewed on NewsMaxTV I explained that a vaccine is made to a specific strain and therefore will be progressively less effective with each succeeding mutation of the virus.
January 24, 2020 Second Interview: Dr Simone discusses How to Prevent the Flu
CORONAVIRUS COVID-19 HAS ALREADY MUTATED
March 5, 2020 – According to scientists in China and published in the National Science Review, coronavirus COVID-19 in China after only a few months has already mutated to a second strain. The two strains are the S type (30%) and the more aggressive L type (70%). Coronaviruses are RNA viruses and mutate often when they replicate quickly. When I was interviewed on NewsMaxTV I explained that a vaccine is made to a specific strain and therefore will be progressively less effective with each succeeding mutation of the virus.

We do not diagnose disease or recommend a dietary supplement for the treatment of disease. Share this information with your physician who can determine what nutrition, disease and injury treatment regimen is best for you.
ACE INHIBITORS, ARBs, IBUPROFEN, THIAZOLIDINEDIONES AND DIABETES MAY CONFER HIGHER RISK FOR COVID-19
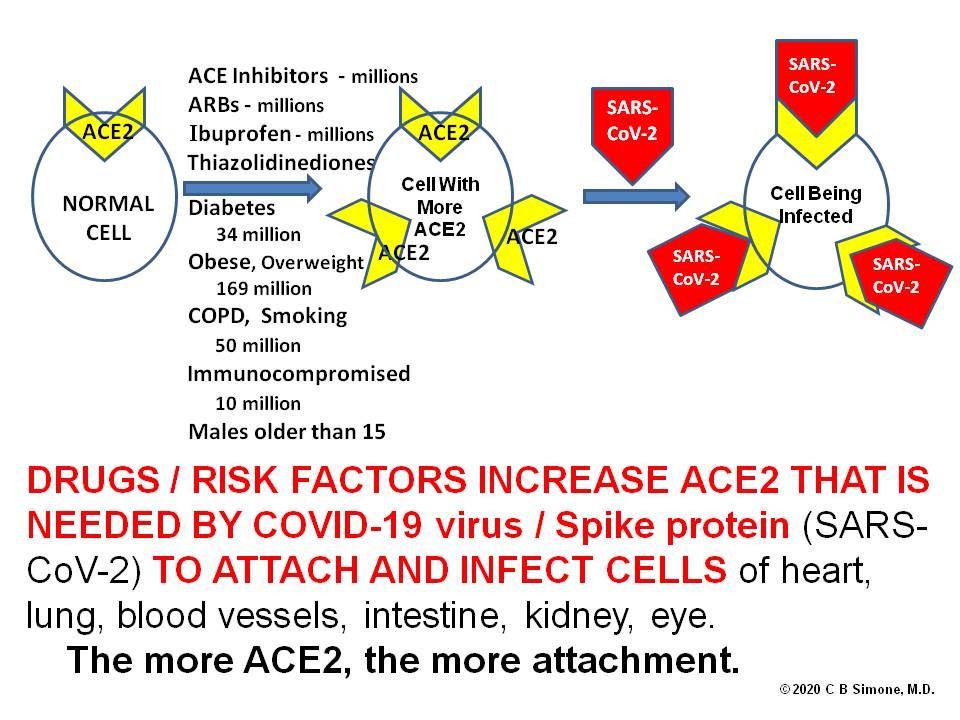
Lawrenceville, NJ (Dr Charles Simone) – It is known that coronaviruses (SARS-CoV – severe acute respiratory syndrome coronavirus, and SARS-CoV-2) bind to target cells via its host receptor angiotensin-converting enzyme 2 (ACE2) [1].
COVID-19 coronavirus attaches and binds to their target cells through ACE2 protein sites on cells of the lung, intestine, kidney, and blood vessels [1].
The most frequent comorbidities (cerebrovascular diseases, diabetes, hypertension, coronary artery disease) reported so far of patients with COVID-19 are usually treated with angiotensin-converting enzyme (ACE) inhibitors, although this was not indicated in the studies.
This higher amount of ACE2 will increase infection with COVID-19 and consequently can increase the risk for severe and fatal COVID-19.
Antihypertensive calcium channel blockers do not increase ACE2 and therefore could be an alternate drug. [3].
[1] Wan Y et al. Receptor recognition by novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS. J Virology. 2020; (published online Jan 29). DOI:10.1128/JVI.00127-20
[2] Li XC et al. The vasoprotective axes of the renin-angiotensin system: physiological relevance and therapeutic implications in cardiovascular, hypertensive and kidney diseases. Pharmacol Res. 2017; 125: 21-38.
[3] Fang L, et al. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respiratory Medicine.3-20
Instead, rely on an empowering plan to protect yourself and your loved ones – go to
FLUhttps://bit.ly/39fGFDz
HOW TO REDUCE YOUR RISK OF CONTRACTING THE FLU? Local governments should implement this PLAN (several steps excerpted with permission)
 |
HOW TO SAVE YOURSELF FROM A TERRORIST ATTACK by Charles B. Simone, M.D.:Pocket size Manual, 48 pages ISBN 0-9714574-1-7 (September 2001) |
We do not diagnose disease or recommend a dietary supplement for the treatment of disease. You should share this information with your physician who can determine what nutrition and disease treatment regimen is best for you.
ENHANCE YOUR IMMUNE SYSTEM to Decrease Your Risk of Infection
Nutrition – Maintain an ideal weight. No four legged animals, shellfish, or dairy products unless they are skim or non-fat. Poultry cooked without the skin. Swimming fish. Fruits and vegetables. Supplement your diet with certain nutrients in the proper doses, chemical form, and correct ratio of one to another. Take high doses of antioxidants (the carotenes, vitamins C and E, selenium, cysteine, copper, zinc, bioflavonoids), the B vitamins, and calcium with its enhancers: magnesium, potassium bicarbonate, boron, L-lysine, silicon, threonine.
Simone Antioxidant – Nutrient Supplementation
Carotene 30 mg Selenium 200 mcg
Lutein 20 mcg Copper 3 mg
Lycopene 20 mcg Zinc 30 mg
Vitamin A 5500 IU Iodine 150 mcg
Vitamin D 400 IU Bioflavonoids 10 mg
Vitamin E 400 IU Chromium 125 mcg
Vitamin C 350 mg Manganese 2.5 mg
Folic Acid 400 mcg Molybdenum 50 mg
All B Vitamins L-Cysteine 20 mg
Tobacco – Do not smoke, chew, snuff, or inhale other people’s smoke
Alcohol – less than 2 drinks per week
Walking – briskly for 20 minutes four times a week.
Modify stress
WASH HANDS AND FACE often with soap. Droplets laden with viruses from people who speak to you travel at least three feet from their mouths. Keep your distance and don’t shake hands. Soap and water is the best. The next best recommended by the Centers for Disease Control and Prevention is a hand sanitizer with at least 60% alcohol and not an alcohol-free hand sanitizer that contains benzalkonium chloride because it may merely reduce the growth of germs rather than kill them.
DROPLET OR AIRBORNE MICROORGANISMS RELEASED FROM VARIOUS ACTIVITIES
ACTIVITY APPROXIMATE PARTICLE COUNT
Sneezing 40,000 Per sneeze
Bowel evacuation 20,000 Per event
Vomiting 1,000 Per event
Coughing 710 Per cough
Talking 36 Per 100 words
Coughing is more common than Sneezing
DECREASE MUCUS PRODUCTION AND MEMBRANE SWELLING by avoiding: Dairy products, citrus, dust mites, air flight, low pressure barometric pressure (rain, snow, overcast weather). Pre-menses swells membranes.

Dust mites live in mattresses, pillows, sheets, blankets, rugs, window dressings, etc. They wait for warm moist bodies – you – and come out by the hundreds of thousands on you, defecate and this causes the allergic reaction that swells sinus exit ports. Use hot water to wash. Cover your mattress and pillows with dust mite covers.
BLEACH – Diluted bleach decontaminates skin and inanimate objects. Viruses generally die on inanimate objects after 12 hours.
Make diluted bleach solution (0.5%) to decontaminate skin from chemicals or biologicals. Even anthrax spores, the most stable of all biologicals, are killed by this solution. Leave this diluted bleach on the skin for about 10-15 minutes. Make this solution by mixing 1 part undiluted bleach from the bottle with 9 parts of water (bleach from the bottle is 5.25%). Make a new solution every day you need it. Avoid eye contact.
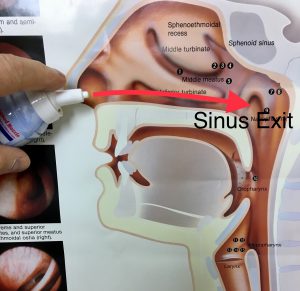
SINUS HYGIENE – Keep sinus exit ports open with:
Steam (10 min every 6 hours),
Oxymetazoline nasal spray that has antiviral effects (over-the-counter https://journals.sagepub.com/doi/10.2500/ajra.2010.24.3491),
Salt water nasal flushes have antiviral effects (https://www.nature.com/articles/s41598-018-37703-3),
Hydration.
SINUS HYGIENE SINUSITIS https://bit.ly/3aiBUsS
Flush your nose with a nasal saline spray to promote mucus flow so that viruses and bacteria can’t lodge. Insert the spray tip in the nostrils perpendicular to the face and direct it toward the ears to get the spray to the exit ports to open them.
Using a syringe bulb, flushes with specific concentrations of over-the-counter Iodine (two teaspoons in 6 ounces of water), or Hydrogen Peroxide, or even very dilute Bleach (several drops in 6 ounces of water) can be used in the same manner as nasal saline. All these flushes are particularly useful if you have been in a crowd or in a high traffic and poorly ventilated public restroom.
Povidone Iodine (PVP-I) Oro-Nasal Spray: An Effective Shield for COVID-19 Protection for Health Care Worker (HCW), for all https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8026810/
Effect of 1% Povidone Iodine Mouthwash/Gargle, Nasal
and Eye Drop in COVID-19 patient file:///C:/Users/mail/Downloads/176-Article%20Text-335-2-10-20210102.pdfThe American Dental Association Council on Dental Therapeutics has designated 0.1% sodium hypochlorite a ‘mild antiseptic mouth rinse’ and suggested its use for direct application to mucous membranes. Dilute sodium hypochlorite has no contraindications. Its high degree of safety permits frequent and broad usage by both dentists and patients.
Effects of 0.05% sodium hypochlorite oral rinse on supragingival biofilm and gingival inflammation https://www.sciencedirect.com/science/article/pii/S0020653920332937Sodium hypochlorite (dilute chlorine bleach) oral rinse in patient self-care
Use steam with Eucalyptus oil – boil about an inch of water in a quart size pot, take it away from the stove, add about 10 drops of Eucalyptus oil, and inhale over the pot with a towel over your head for about ten minutes four to five times a day. You may use an over-the-counter Oxymetazoline nasal spray (not a banned substance) as directed. You can add a prescription steroid nasal spray to keep inflammation down but this requires a Therapeutic Use Exemption approval during sports competitions. Insert the spray tip in the nostrils perpendicular to the face and direct it toward the ears to get the medicine to the exit ports to open them. Hydrate to keep the mucus thin and flowing.
HYDROGEN PEROXIDE changes the structure of viruses and generates oxygen that kills viruses. Gargle for several minutes with hydrogen peroxide (right from the bottle) twice a day.
ZINC – weekly dose of 70 mg for all ages reduces mortality/morbidity from viruses and bacteria*. Also, Zinc Lozenges.
*1) Brooks WA, et al. Lancet. 2005. 366:999-1004. 2) Bhatnagar S. Lancet. 2007. 369:885-886. 3) Sazawal S et al. Lancet. 2007. 369:927-34. 4) Barnett J, Nutr Rev 2010 Jan 68(1):30-37
N-ACETYL CYSTEINE 600 mg twice a day.
VITAMIN C 2 to 4 gm & VITAMIN D 5000 IU per day.
QUERCETIN 500 mg twice per day (nutrient over-the-counter) – interferes with the virus binding onto your cells.
Quercetin possesses anti-influenza activity by inhibiting viral entry, viral-cell fusion, viral replication, viral load, and lung inflammation and airways hyper-responsiveness in vivo. Quercetin has strong antibacterial, antifungal and antiviral properties.
Wenjiao W, et al. Viruses. 2016. Jan. 8(1):6; Kinker et al. J Infectious Diseases & Preventive Med 2014 2.2.
A reduction in total sick days and severity was noted in middle aged and older subjects ingesting 1000 mg quercetin per day for 12 weeks who rated themselves as physically fit (Heinz SA et al. Pharmacol Res. 2010 Sep;62(3):237-42).
Quercetin outperforms Tamiflu – A mouse study showed that quercetin reduced symptoms and gave higher survival rates. Also, animals treated with Quercetin had half of the virus load in their lungs compared to animals treated with Tamiflu. (Choi HJ, et al. Phytother Res. 2012 Mar;26(3):462-4).
Tamiflu’s chemical structure is similar to Quercetin but different enough to allow it to be patented. Despite all the media attention about Tamiflu, here is what the makers of Tamiflu say in their insert (Nov ’09):
Adults felt better 30 percent faster (1.3 days) than flu patients who did not take TAMIFLU
Children felt better up to 26 percent faster (1.5 days) than flu patients who did not take TAMIFLU

